Caremark Medicare Prior Authorization Form
Caremark Medicare Prior Authorization Form - If a form for the specific medication cannot be found, please use the global prior authorization form. California members please use the. Contact us to learn how to name a representative. Attach documentation showing the authority to represent the enrollee (a completed. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the.
If a form for the specific medication cannot be found, please use the global prior authorization form. Attach documentation showing the authority to represent the enrollee (a completed. California members please use the. Contact us to learn how to name a representative. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the.
Contact us to learn how to name a representative. Attach documentation showing the authority to represent the enrollee (a completed. California members please use the. If a form for the specific medication cannot be found, please use the global prior authorization form. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the.
Prior Authorization Form For Medicare Part B Form Resume Examples
If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the. Contact us to learn how to name a representative. California members please use the. Attach documentation showing the authority to represent the enrollee (a completed. If a form for the specific medication cannot be found, please use the global.

Caremark Medicare Part D Medication Prior Authorization Form Form
Attach documentation showing the authority to represent the enrollee (a completed. Contact us to learn how to name a representative. California members please use the. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the. If a form for the specific medication cannot be found, please use the global.
FREE 8+ Sample Caremark Prior Authorization Forms in PDF
Contact us to learn how to name a representative. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the. Attach documentation showing the authority to represent the enrollee (a completed. If a form for the specific medication cannot be found, please use the global prior authorization form. California members.
Medicare Part B Prior Authorization Form Form Resume Examples
Contact us to learn how to name a representative. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the. Attach documentation showing the authority to represent the enrollee (a completed. California members please use the. If a form for the specific medication cannot be found, please use the global.

Cvs Caremark Wegovy Prior Authorization Form
California members please use the. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the. If a form for the specific medication cannot be found, please use the global prior authorization form. Contact us to learn how to name a representative. Attach documentation showing the authority to represent the.
Cvs Caremark Appeal PDF 20032024 Form Fill Out and Sign Printable
If a form for the specific medication cannot be found, please use the global prior authorization form. Contact us to learn how to name a representative. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the. California members please use the. Attach documentation showing the authority to represent the.
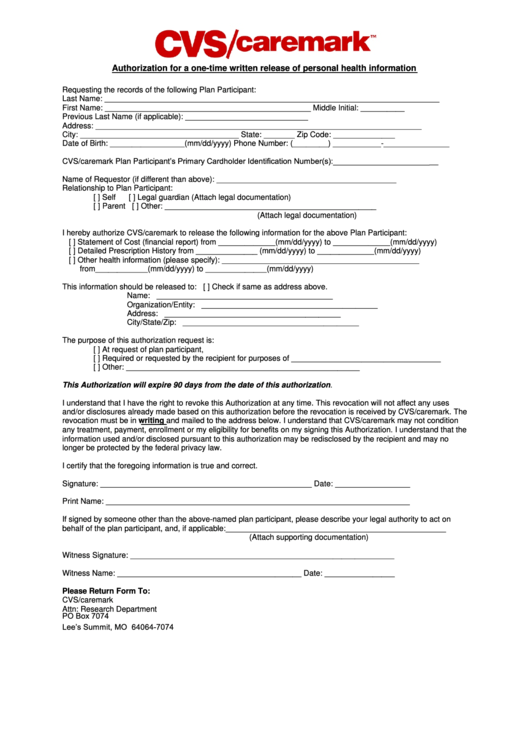
Authorization For A Written Release Of Personal Health
Attach documentation showing the authority to represent the enrollee (a completed. Contact us to learn how to name a representative. If a form for the specific medication cannot be found, please use the global prior authorization form. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the. California members.
Template Caremark Prior Authorization Form Mous Syusa
California members please use the. Contact us to learn how to name a representative. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the. If a form for the specific medication cannot be found, please use the global prior authorization form. Attach documentation showing the authority to represent the.
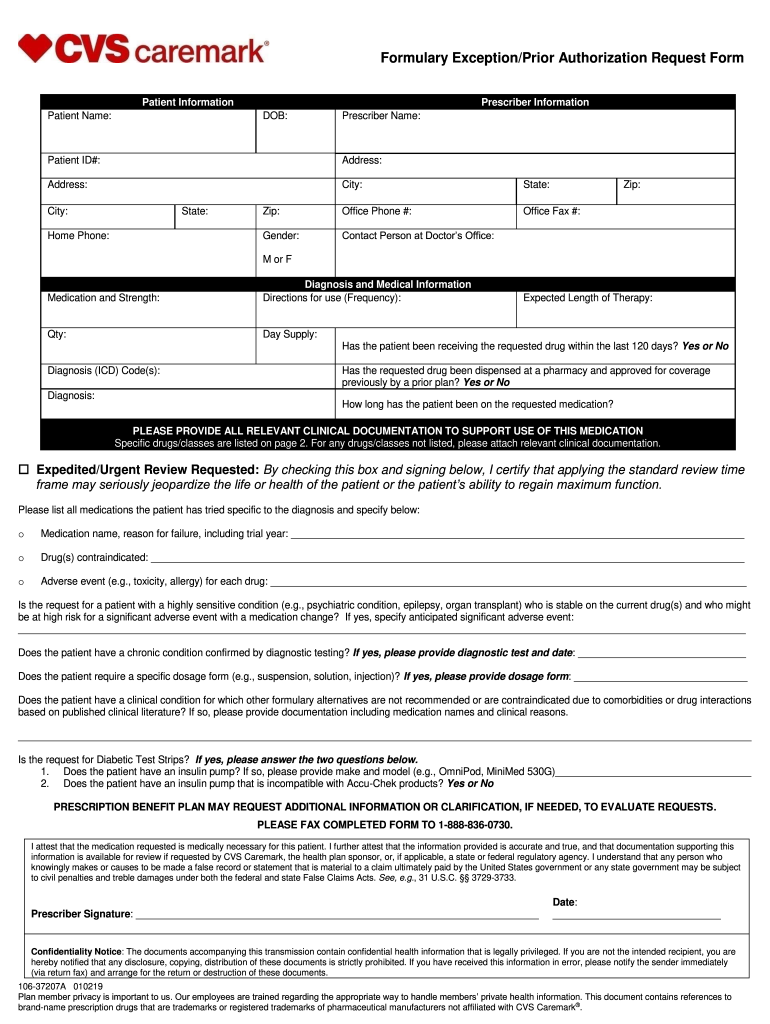
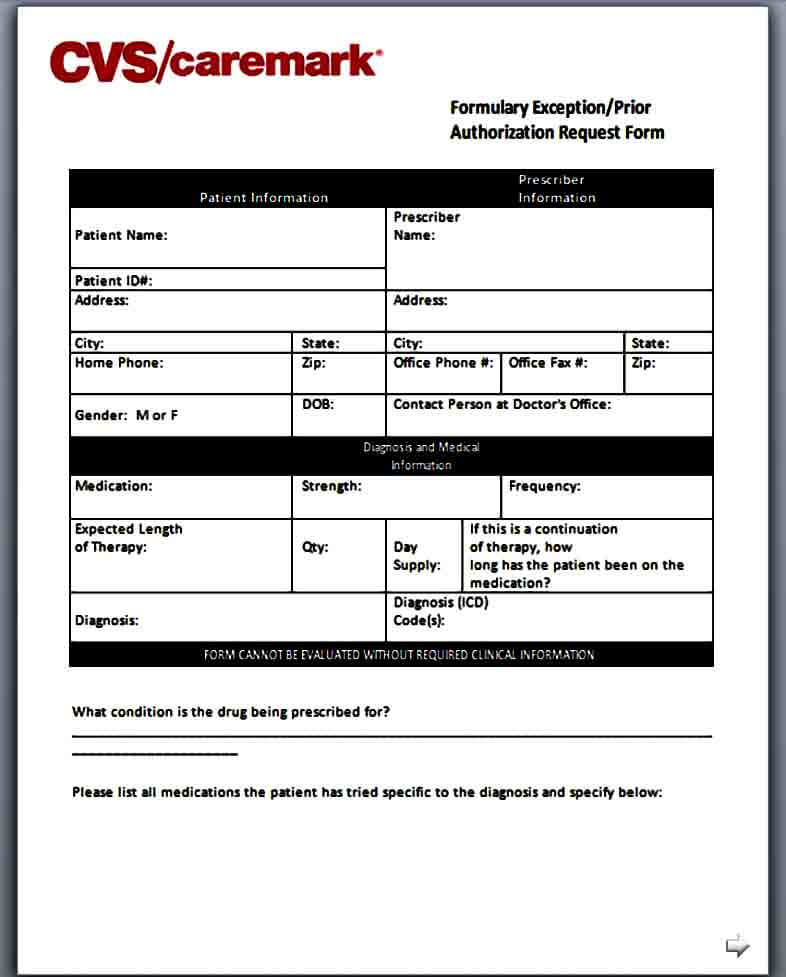
Formulary ExceptionPrior Authorization Request Form Fill Out and Sign
If a form for the specific medication cannot be found, please use the global prior authorization form. Attach documentation showing the authority to represent the enrollee (a completed. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the. Contact us to learn how to name a representative. California members.

20202024 Form NY Healthfirst Request for Medicare Prescription Drug
If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the. Attach documentation showing the authority to represent the enrollee (a completed. California members please use the. If a form for the specific medication cannot be found, please use the global prior authorization form. Contact us to learn how to.
Contact Us To Learn How To Name A Representative.
If a form for the specific medication cannot be found, please use the global prior authorization form. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the. Attach documentation showing the authority to represent the enrollee (a completed. California members please use the.