Florida Bcbs Appeal Form
Florida Bcbs Appeal Form - When submitting a provider reconsideration or administrative appeal, please complete the form in its entirety in accordance with the. Provider clinical appeal form when submitting a provider appeal, please complete the form in its entirety in accordance with the instructions. Correspondence will be sent directly to the benefit address we have on file for the member referenced in the appeal. If you are looking to file a health or dental claim, you can do so by logging into my health toolkit. Once logged in, look under claims &.
Provider clinical appeal form when submitting a provider appeal, please complete the form in its entirety in accordance with the instructions. Once logged in, look under claims &. When submitting a provider reconsideration or administrative appeal, please complete the form in its entirety in accordance with the. Correspondence will be sent directly to the benefit address we have on file for the member referenced in the appeal. If you are looking to file a health or dental claim, you can do so by logging into my health toolkit.
When submitting a provider reconsideration or administrative appeal, please complete the form in its entirety in accordance with the. Once logged in, look under claims &. Correspondence will be sent directly to the benefit address we have on file for the member referenced in the appeal. If you are looking to file a health or dental claim, you can do so by logging into my health toolkit. Provider clinical appeal form when submitting a provider appeal, please complete the form in its entirety in accordance with the instructions.

Fillable Online Bcbs provider appeal form michigan. Bcbs provider
Provider clinical appeal form when submitting a provider appeal, please complete the form in its entirety in accordance with the instructions. Correspondence will be sent directly to the benefit address we have on file for the member referenced in the appeal. When submitting a provider reconsideration or administrative appeal, please complete the form in its entirety in accordance with the..
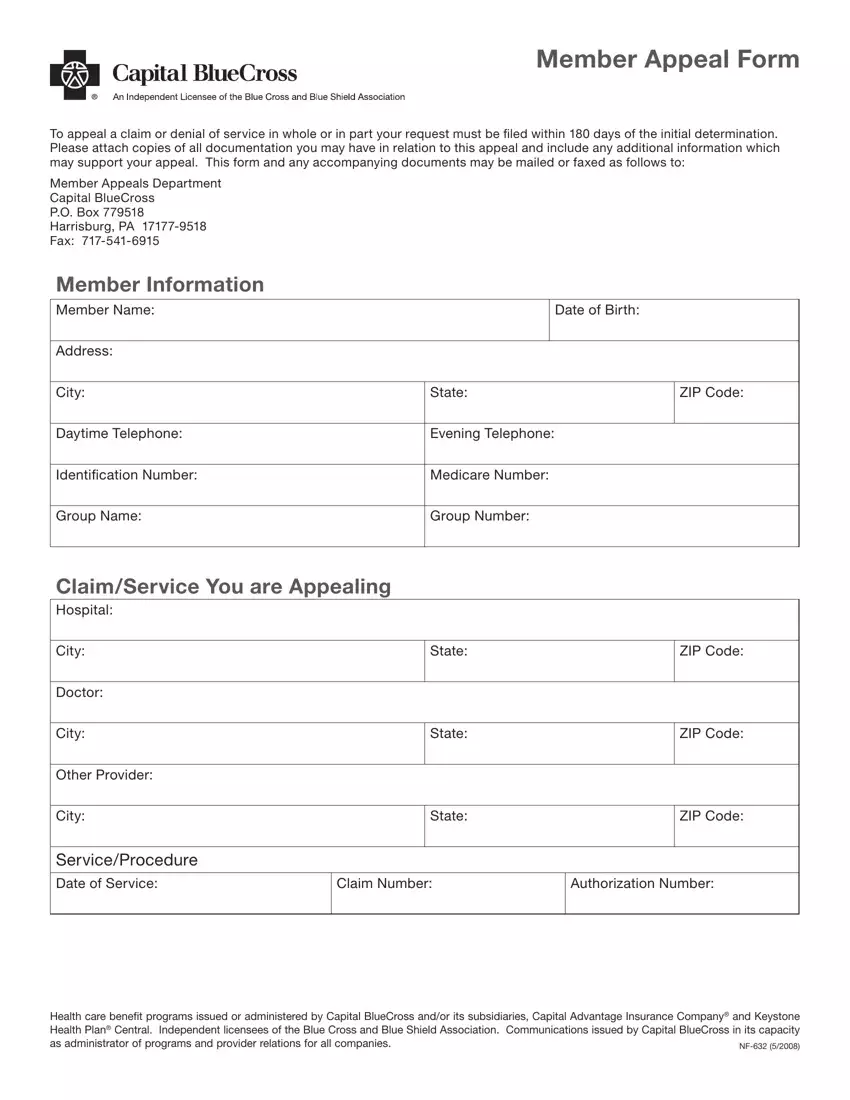
Capital Blue Cross Provider Appeal PDF Form FormsPal
When submitting a provider reconsideration or administrative appeal, please complete the form in its entirety in accordance with the. Once logged in, look under claims &. Provider clinical appeal form when submitting a provider appeal, please complete the form in its entirety in accordance with the instructions. If you are looking to file a health or dental claim, you can.
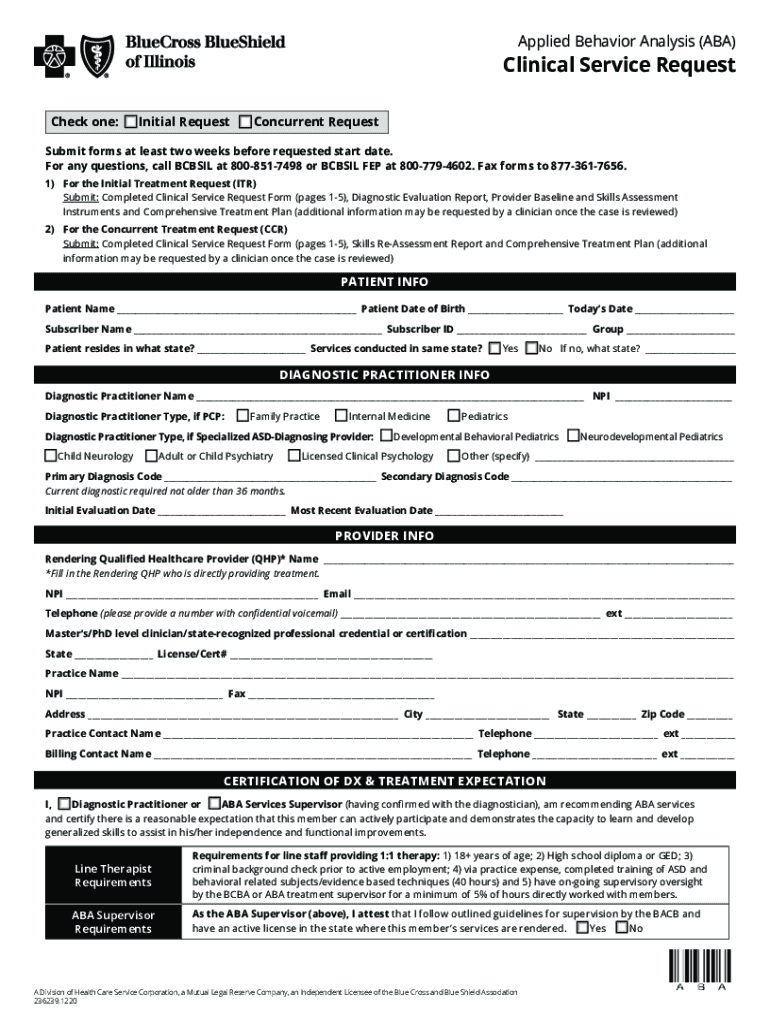
Clinical Request Form Complete with ease airSlate SignNow
If you are looking to file a health or dental claim, you can do so by logging into my health toolkit. Provider clinical appeal form when submitting a provider appeal, please complete the form in its entirety in accordance with the instructions. When submitting a provider reconsideration or administrative appeal, please complete the form in its entirety in accordance with.

Fillable Online Bcbs Federal Employee Program Provider Appeal Form
Once logged in, look under claims &. Correspondence will be sent directly to the benefit address we have on file for the member referenced in the appeal. If you are looking to file a health or dental claim, you can do so by logging into my health toolkit. When submitting a provider reconsideration or administrative appeal, please complete the form.
Appeal Form Template
If you are looking to file a health or dental claim, you can do so by logging into my health toolkit. Once logged in, look under claims &. When submitting a provider reconsideration or administrative appeal, please complete the form in its entirety in accordance with the. Provider clinical appeal form when submitting a provider appeal, please complete the form.

BCBS Florida Medical Policy Updates July 2021
Once logged in, look under claims &. Provider clinical appeal form when submitting a provider appeal, please complete the form in its entirety in accordance with the instructions. If you are looking to file a health or dental claim, you can do so by logging into my health toolkit. When submitting a provider reconsideration or administrative appeal, please complete the.
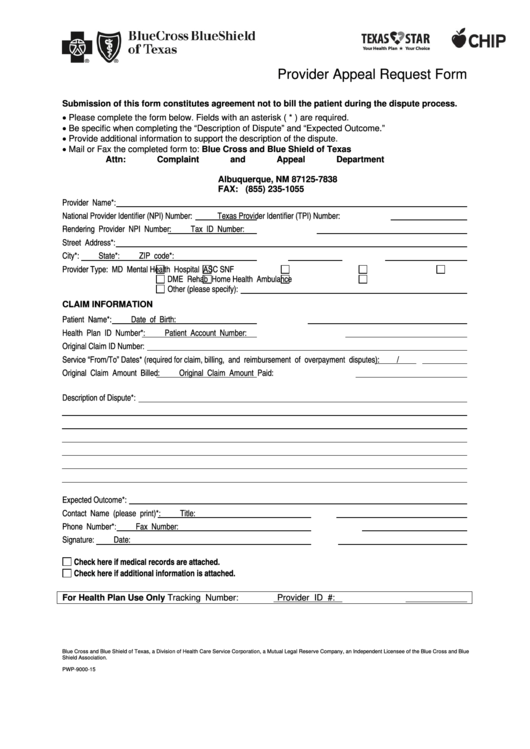
Bluecross Blueshield Of Texas Provider Appeal Request Form printable
Provider clinical appeal form when submitting a provider appeal, please complete the form in its entirety in accordance with the instructions. Once logged in, look under claims &. When submitting a provider reconsideration or administrative appeal, please complete the form in its entirety in accordance with the. If you are looking to file a health or dental claim, you can.
Standard authorization form bcbs Fill out & sign online DocHub
When submitting a provider reconsideration or administrative appeal, please complete the form in its entirety in accordance with the. Provider clinical appeal form when submitting a provider appeal, please complete the form in its entirety in accordance with the instructions. If you are looking to file a health or dental claim, you can do so by logging into my health.
Blue Shield Bcbs Of Texas Prior Authorization Form
If you are looking to file a health or dental claim, you can do so by logging into my health toolkit. Provider clinical appeal form when submitting a provider appeal, please complete the form in its entirety in accordance with the instructions. When submitting a provider reconsideration or administrative appeal, please complete the form in its entirety in accordance with.

20202024 Sunshine Health Inpatient Medicaid Prior Authorization Fax
Once logged in, look under claims &. Correspondence will be sent directly to the benefit address we have on file for the member referenced in the appeal. When submitting a provider reconsideration or administrative appeal, please complete the form in its entirety in accordance with the. Provider clinical appeal form when submitting a provider appeal, please complete the form in.
Provider Clinical Appeal Form When Submitting A Provider Appeal, Please Complete The Form In Its Entirety In Accordance With The Instructions.
Correspondence will be sent directly to the benefit address we have on file for the member referenced in the appeal. When submitting a provider reconsideration or administrative appeal, please complete the form in its entirety in accordance with the. If you are looking to file a health or dental claim, you can do so by logging into my health toolkit. Once logged in, look under claims &.